Aplikacija Moj križ je odlično dopolnilo k vaši fizioterapiji. Aplikacija ne nadomešča vašega fizioterapevta ali fizioterapevtskih vaj. Aplikacija je rezultat lastnih izkušenj (fizioterapij, športnih aktivnosti, itd) in študija literature opisane v blogu .
Preden začnete z vadbo se posvetujte z vašim zdravnikom o primernosti vaj za vas, še posebej, če se s podobnimi vajami še niste srečali.
200Aplikacija Moj križ omogoča osnovno navigacijo : – glavni meni, – spletni dostop do http://biofit.blog/ – nastavitne aplikacije in – izhod.
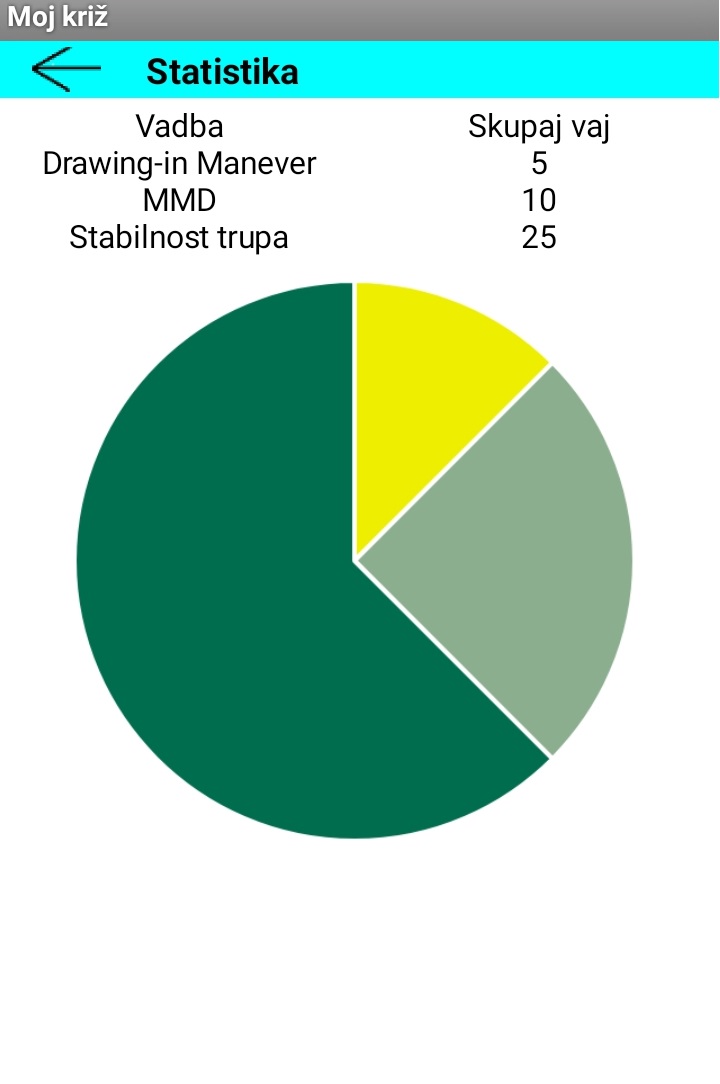
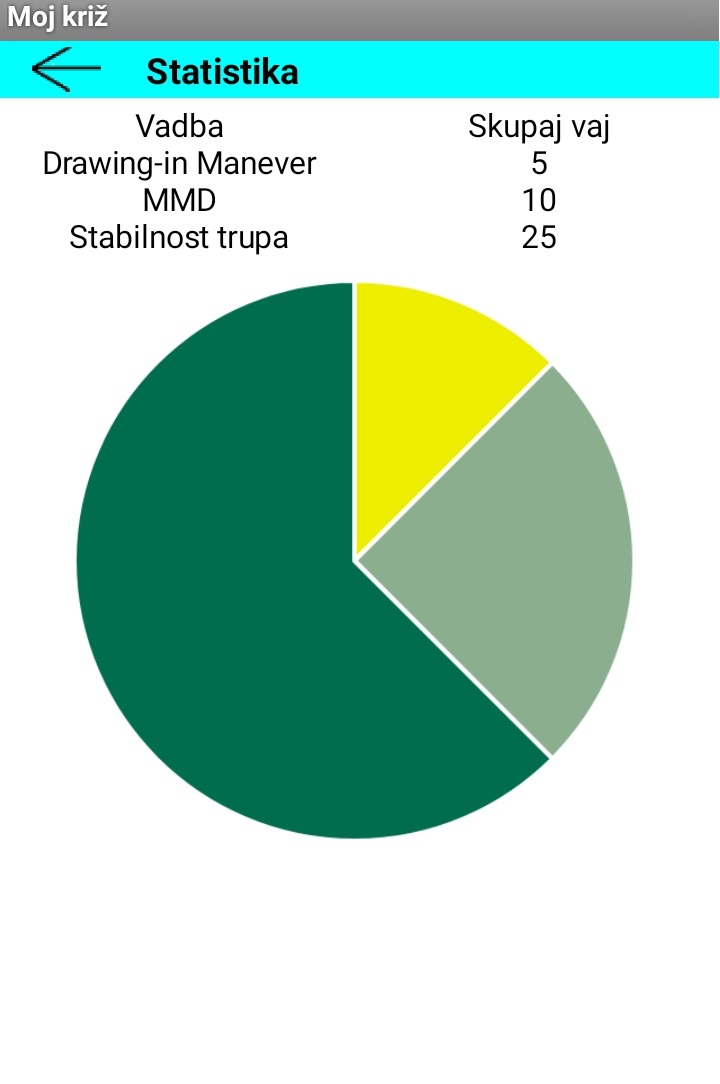
Napredna navigacija omogoča : – izbiro vadbenega programa, – statistiko: grafični prikaz opravljenih vaj – informacije o aplikaciji.
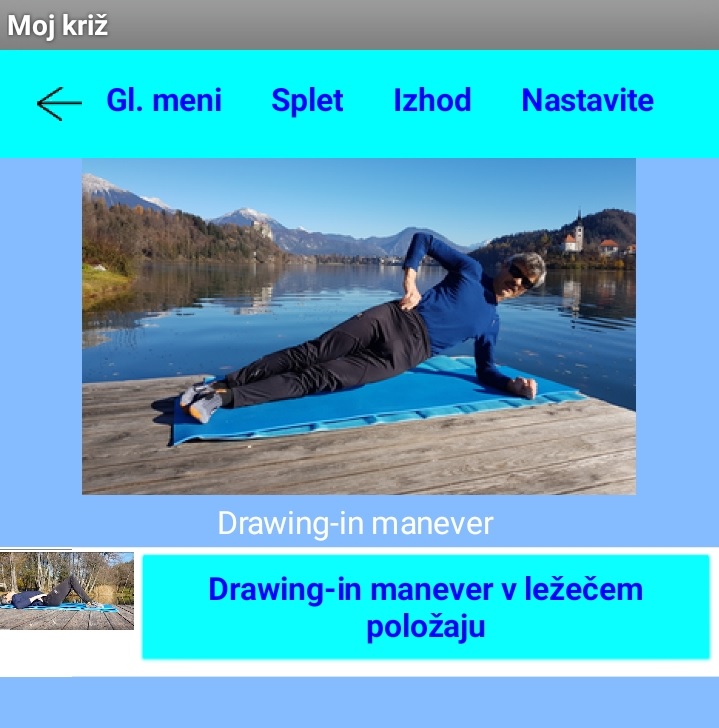
Osnovna vaja je drawing-in manever v ležečem položaju s katero napnemo mišice trupa in mišice medeničnega dna (MMD). Ta vaja je osnova in začetek za vsako naslednjo vajo.
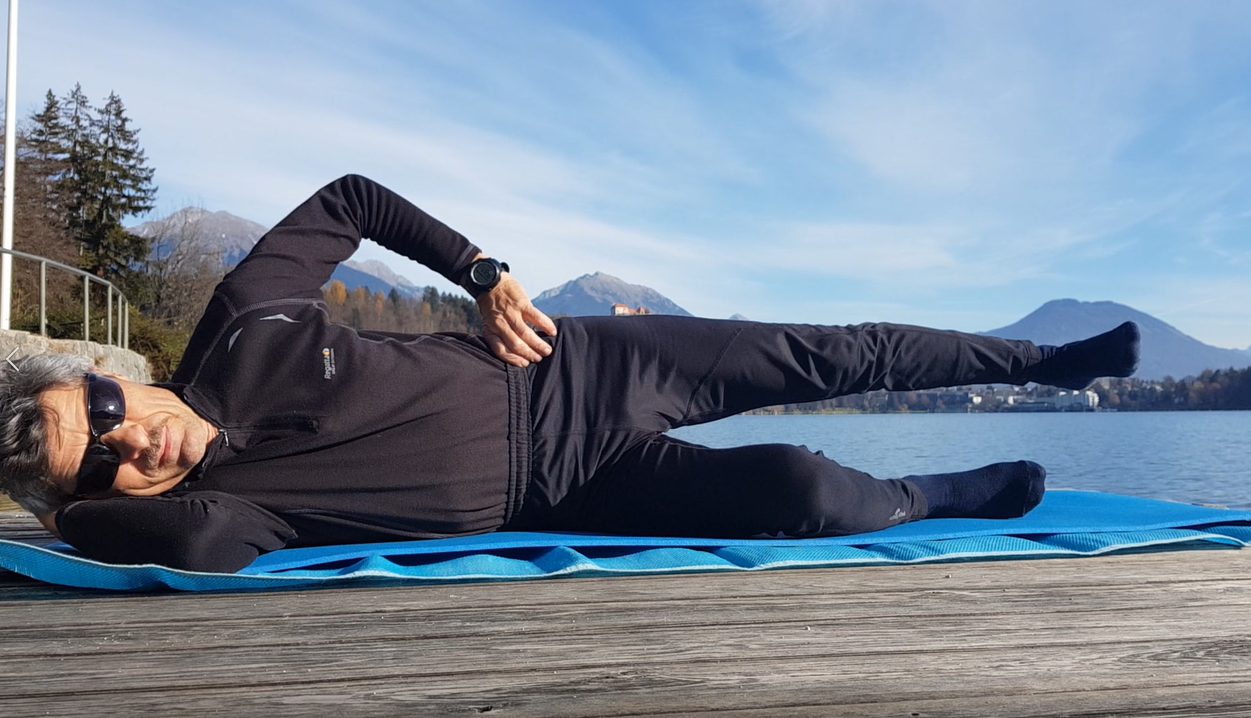
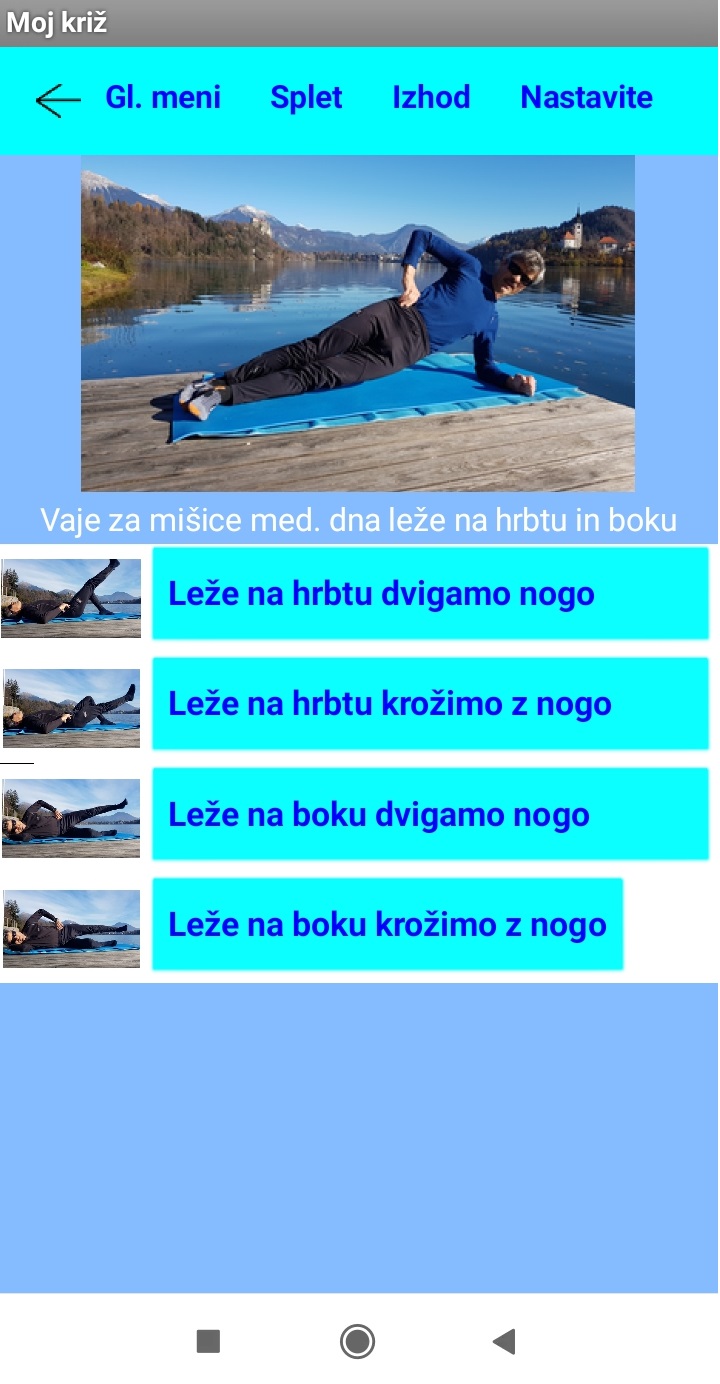
Vaja za mišice medeničnega dna sestavljajo vaje leže na hrbtu in boku s katerimi ojačamo predvsem mišice medeničnega dna (MMD)
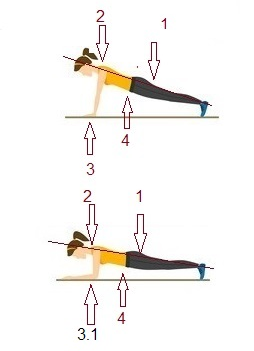
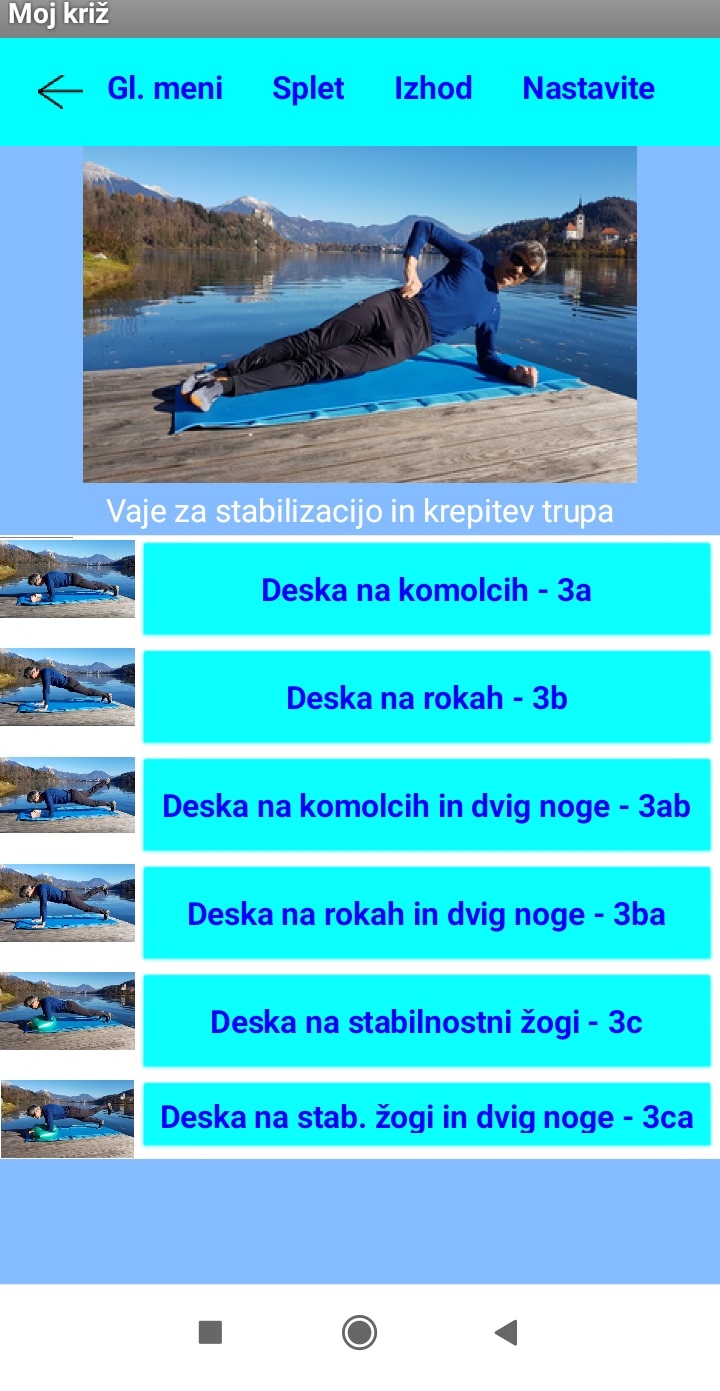
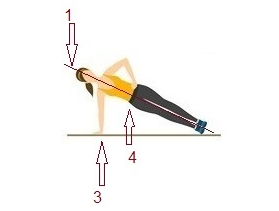
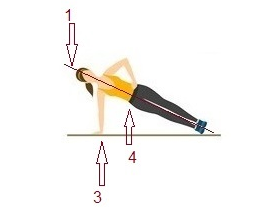
Prilagojena stranska deska je namenjena stabilizaciji trupa in krepitvi trupa.Pravilna izvedba telovadne deske: 1- stisnite zadnjico, oblikujte pravi položaj deske v ravni črti od prstov, skozi boke, do vratu 3- ramena neposredno nad zapestji 4- okrepite svoj trup, tako da stisnite trebušne mišice in mišice trupa
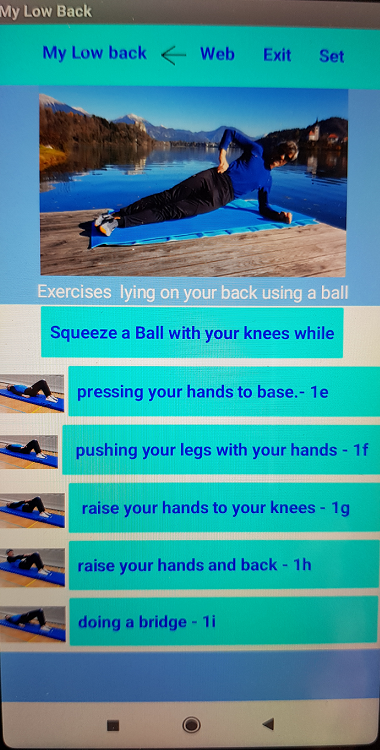
Vaje leže na hrbtu z žogo so namenjene raztezanju mišic trupa in ojačanju mišic medeničnega dna (MMD).
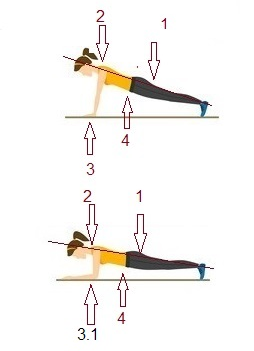
Vaja “telovadna deska” omogoča krepitev mišic trupa. Pravilna izvedba telovadne deske: 1- stisnite zadnjico, oblikujte pravi položaj deske v ravni črti od prstov, skozi boke, do vratu 2-vrat naj bo v liniji s hrbtenico linija gre naravnost od ušesia, ramen, bokov in do pete 3-ramena neposredno nad zapestji 3.1-komolci neposredno pod rameni 4-okrepite svoj trup, tako da stisnite trebušne mišice in mišice trupa
Statistika omogoča grafičen prikaz opravljenih vaj. Statistika združuje vaje so po sklopih: – drawing-in manever, – vaje za stabilizacijo trupa, – vaje za mišice mediničnega dna (MMD) – vaje z žogo, – vaje leže na hrbtu za MMD), – vaje za stabilizacijo in krepitev trupa
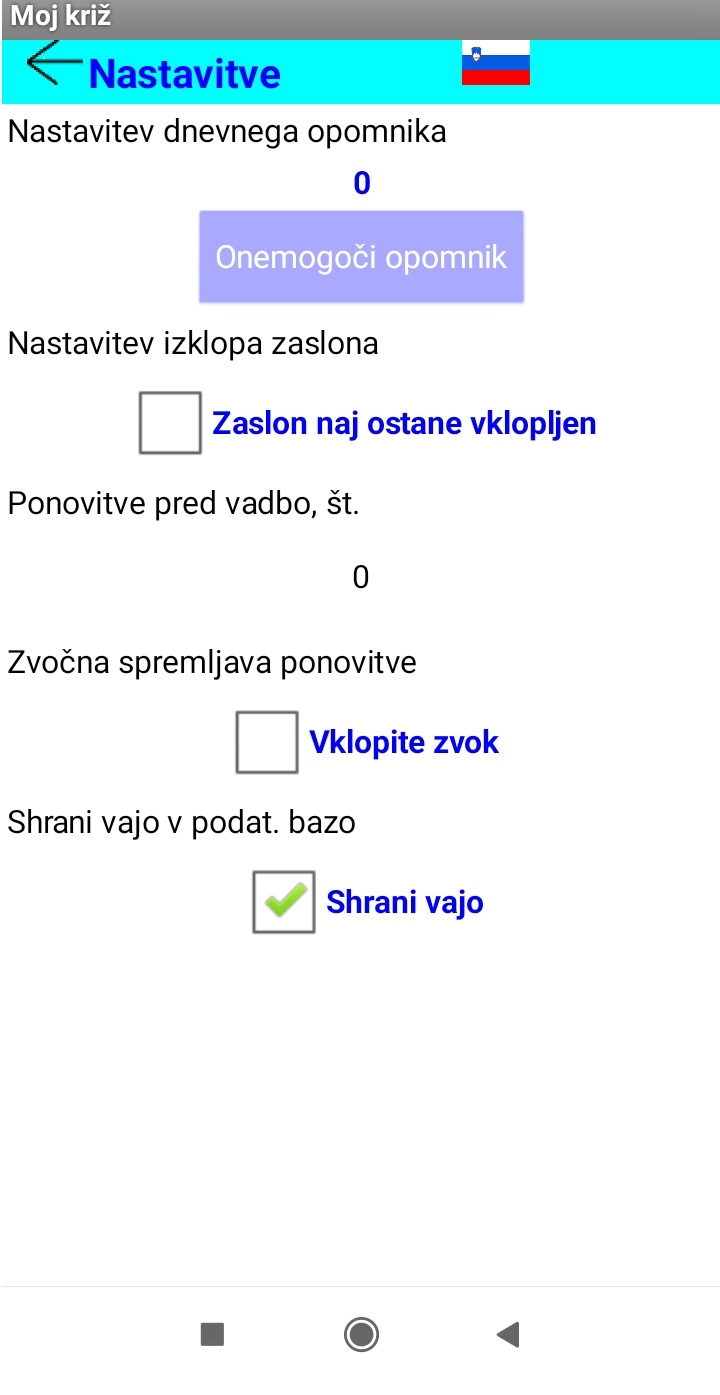
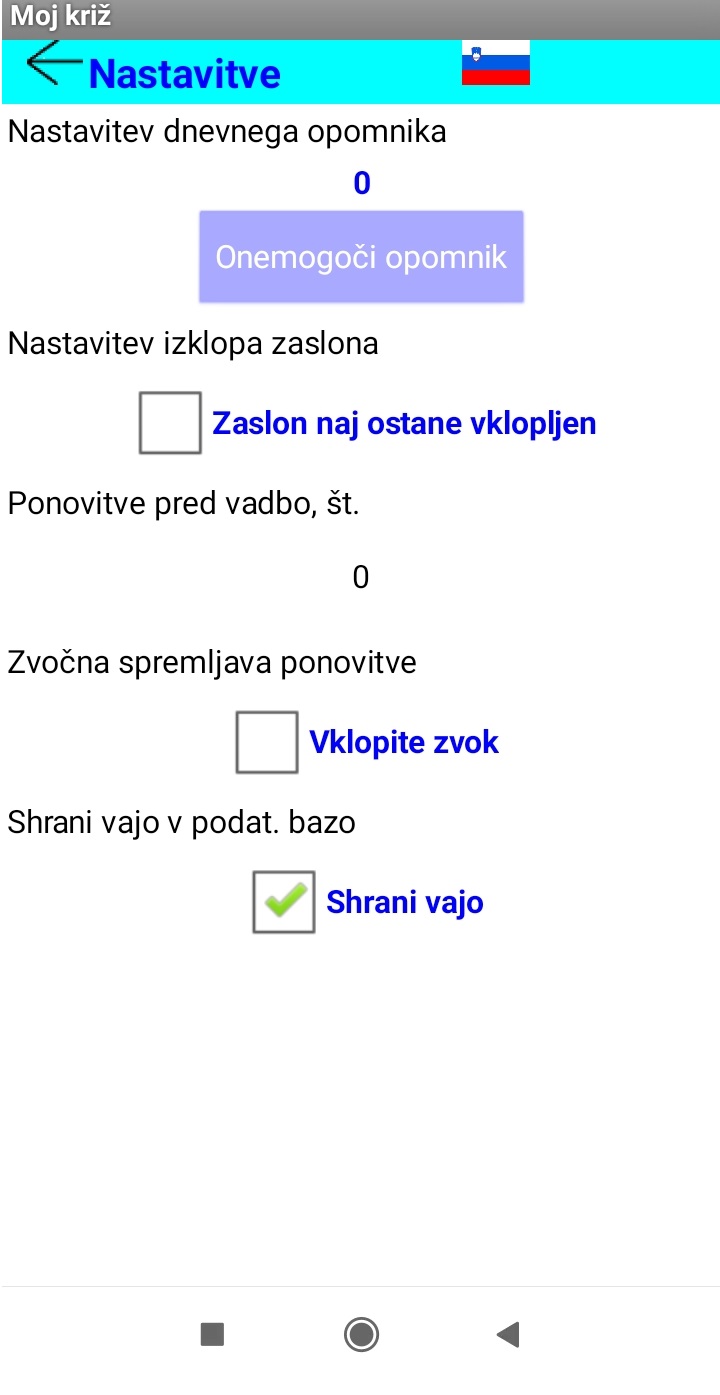
Nastavitve omogočajo izbiro jezika : – angleško , – slovensko Nastavitev dnevnega opomnika omogoča nastavitev alarma telefona. Če v telefonu izključimo alarm, ta nastavitev ni več aktualna. Nastavitev zaslona omogoča, da se zaslon ne izklopi oziroma ne gre v mirovanje. Ponovitve pred vadbo omogoča pripravo na vadbo . Zvočna spremljava omogoča pisk za začetek izvajanja vadbe in začetek mirovanja. Shrani vajo v podatkovno bazo omogoča zapis števila vadb za kasnejši grafični prikaz
1. PFM Exercises lying on your back and side, dificulty : light (PFM _ back _side) label25
Exercise
Description
Starting position
1a
Lying down on your back, one leg bent and the other one streched, stable lumbar region, execution of a drawing-in maneuver. Raise outstretched leg (pain-free)
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week 4: 5 Both(L+R):Y
1b
Lying down on your back ,one leg bent and the other one stretched, stable lumbar region, execution of a drawing-in maneuver, Circle with the leg streched (pain-free).
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week 4: 5 Both(L+R):Y
1c
Lying down on your side, one leg bent and the other one stretched, stable lumbar region, execution of a drawing-in maneuver, Raise outstretched leg(pain-free)
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week 4: 5 Both(L+R):Y
1d
PFM Exercises, lying on your back circling your leg. Lying down on your side, one leg bent and the other one stretched, stable lumbar region, execution of a drawing-in maneuver. Circle with the stretched leg (pain-free).
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week 4: 5 Both(L+R):Y
1. Repetition: The number of repetitions of the exercise, if L + D, is the number of repetitions for each leg
2. Duration: duration in seconds or holding positions
3. Break: Leave during exercise for a few seconds.
4. Days of the week: number of training days per week
The duration of the activation period of local stabilizers will vary for the patients. People differ in their abilities. Some will master activation techniques earlier, others later, however, it is recommended to perform at least four weeks of exercise to activate the abdominal muscles and pelvic floor muscles. Only the correct execution of the drawing-in maneuver can allow us to safely perform all exercises to stabilize the core in the following periods, which in turn can lead us to reduce low back pain. Also very important is the development of the pelvic floor muscles, to which most people pay too little attention.
1. PFM Exercises lying on your back using a ball.
Exercise
Description
Starting position
1e
Lying down on your back, legs bent, stable lumbar region, execution of a drawing-in maneuver, squeeze a ball with your knees and press your hands to base. Equipment: ball.
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week 4: 5 Both(L+R) :Y
1f
Lying down on your back, legs bent, stable lumbar region, execution of a drawing-in maneuver, squeeze a ball with your knees and push your legs with your hands. Equipment: ball.
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week 4: 5 Both(L+R) :Y
1g
Lying down on your back, legs bent, stable lumbar region, execution of a drawing-in maneuver, squeeze a ball with your knees and raise your hands to your knees. Equipment: ball.
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week 4: 5 Both(L+R):Y
1h
Lying down on your back, legs bent, stable lumbar region, execution of a drawing-in maneuver, squeeze a ball with your knees and raise your back and hands to your knees . Equipment: ball.
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week 4: 5 Both(L+R):Y
1i
Lying down on your back, legs bent, stable lumbar region, execution of a drawing-in maneuver, squeeze a ball with your knees while doing a bridge with your back. Equipment: ball.
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week 4: 5 Both(L+R):Y
1j
Lying down on your back, legs bent, stable lumbar region, execution of a drawing-in maneuver, squeeze a ball with your knees while pushing your knees away with your hands. Equipment: ball.
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week 4: 5 Both(L+R):Y
2. Core stabilization exercises
2.1 Core stabilization exercises in kneeling a position (menu_second_core_stab)
Exercise
Description
Starting position
2a
On Hands & Knees Leg Lift The support in is on the hands, and knee, toe and outstretched leg, stable lumbar region, execution of a drawing-in maneuver, Raise outstretched leg Equipment: stick Core stabilization-2a-desna.mp4 Core stabilization-2a-leva.mp4
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week 4: 5 Both(L+R):Y
2b
On Hands & Knees Arm/Leg Lift The support in is on the hands, knee and toe, leg is outstretched, stable lumbar region, execution of a drawing-in maneuver. Raise outstretched leg and oposite arm. Equipment:stick Core stabilization-2b-desna.mp4 Core stabilization-2b-leva.mp4
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week4:5 Both(L+R):Y
2.2 Core stabilization exercises in side position
2c
Modified side plank, lift hip lying down on your side, one leg bent and the other one streched, stable lumbar egion, execution of a drawing-in maneuver. Raise your hip Core stabilization-2c.mp4 Core stabilization-2c-still.mp4
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week4:5 Both(L+R):Y
2b
Modified Side Plank, leg circling, lying down on your side, one leg bent and the other one streched, stable lumbar egion, execution of a drawing-in maneuver. Raise your hip and outstretched leg Core stabilization-2d1.mp4 Core stabilization-2d2.mp4
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week4:5 Both(L+R):Y
2d
Modified Side Plank, leg circling , lying down on your side, one leg bent and the other one streched, stable lumbar egion, execution of a drawing-in maneuver. Raise your hip and circle your outstretched leg Core stabilization-2d1.mp4 Core stabilization-2d2.mp4
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week4:5 Both(L+R):Y
2e
Walking with sticks. Equipment: sticks
Duration: 1 h Daily(Y/N): Y
3. Core stabilization and strengthen exercises
3a
Elbow plank/Forearm plank The support in is on the elbows, knee and toe , stable lumbar region, execution of a drawing-in maneuver. Raise your hip. core strength-3a-still.mp4 core strength-3a-desna.mp4 core strength-3a-leva.mp4
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week 4: 5 Both(L+R):Y
3b
Elbow plank/Forearm plank The support in is on the elbows and toes , stable lumbar region, execution of a drawing-in maneuver. Raise one leg. core strength-3a-still.mp4 core strength-3a-desna.mp4 core strength-3a-leva.mp4
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week 4: 5 Both(L+R):Y
3c
Hand plank The support in is on the hands , knee and toe, stable lumbar region, execution of a drawing-in maneuver. Raise hip. core strength-3b-desna.mp4 core strength-3b-leva.mp4 core strength-3b-stil.mp4
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week 4: 5 Both(L+R):Y
3d
Hand plank The support in is on the hands, knee and toe, stable lumbar region, execution of a drawing-in maneuver. Raise the leg. core strength-3b-desna.mp4 core strength-3b-leva.mp4 core strength-3b-stil.mp4
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week 4: 5 Both(L+R):Y
3.1 Core stabilization and strengthen exercises using stability ball
3e
Stability ball elbow plank The support in is on the elbows and toes , stable lumbar region, execution of a drawing-in maneuver. Alternative Raise the leg. Equipment: ball. Core Strength-3c-desna.mp4 Core Strength-3c-leva.mp4 Core Strength-3c-stil.mp4
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week 4: 5 Both(L+R) :Y
3f
Stability ball elbow plank The support in is on the elbows and toes , stable lumbar region, execution of a drawing-in maneuver. Alternative Raise the leg. Equipment: ball. Core Strength-3c-desna.mp4 Core Strength-3c-leva.mp4 Core Strength-3c-stil.mp4
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week 4: 5 Both(L+R) :Y
3g
Stability ball elbow side plank The support in is on the elbow and toes , hip is on base, stable lumbar region, execution of a drawing-in maneuver. Raise your hip. Equipment: ball.
Repetition 1 : 5 x Duration 2 : 5 sek Break 3 : 5 sek Days of the week 4: 5 Both(L+R):Y
The main purpose of this paper is to design a comprehensive exercise program for development of core strength and stability in patients with lumbago. I conduct an extensive and thorough analytical literature review of the existing research on the topic and developed the exercise program that helps to reduce and in some cases eliminate the pain in the lower back region.
We provide explanation of muscles important for low back and low back pain relief. Next we explain pelvic floor muscles, that take care of the correct position of the pelvic organs, and at the same time stabilize the spine.
Lastly, in developing my own exercise program, the program is methodically divided into three consecutive segments. For each segment, we propound a basic and a more advanced set of exercises in order to account for the differences in physical fitness level of the patients.
1.0 Low back pain
According to some estimates, between 60% and 80% of people experience back pain at least once in their lifetime. Most of these pains occur in the lower or lumbar spine. Due to back problems and pain, on average, each worker loses three working days a year.
To summarize some research in McGill (2007), they say that people with past lower back pain and problems have been associated with increased waist circumference, decreased muscle capacity, especially core muscles, decreased hip mobility in extension and internal rotation, and deficient motion control. In his book, McGill (2007) also summarizes in vitro testing for the causes of injuries, proposing that a reduction in specific tissue damage can be achieved with the following recommendations:
elimination of stressors that cause damage to the lumbar spine,
implementation of activities for healthy supporting tissue,
the ideal sitting posture is one that is constantly changing but still prevents the tissue from too burdened;
there are two types of risk factors that people have a predisposition to develop lower back problems:
these are those factors that are related to the person (e.g., a person’s muscular endurance or lack of endurance) and those
that are related to the requirements of the task we need to perform (e.g., lifting weights, loading a load, etc.).
Low back pain needs to be addressed from several perspectives. A distinction must be made between
acute lumbalgia lasting less than six weeks,
subacute lumbalgia lasting between six weeks and twelve weeks and
chronic lumbalgia lasting more than twelve weeks.
Low back pain needs to be addressed from several perspectives. A distinction must be made between acute lumbalgia lasting less than six weeks and chronic lumbalgia lasting more than twelve weeks. The causes of most acute, short-term low back pain are mechanical or nonspecific, especially minor injuries to the spinal muscles and ligaments, unphysiological position in the workplace, poor posture, excessive sports and other loads, congenital and acquired spinal anomalies. Acute low back pain usually passes quickly, especially after the removal of triggers (Kos, Golja, 2001).
The eternal question is also whether to rest during the pain in the upper or lower back or to move rather. There has long been a belief that the best treatment and recovery for low back pain is prolonged rest or lying down. However, lying in bed for more than two days only harms the situation as the bones and muscles become weaker, the body becomes stunted, loses physical strength, the person may fall into depression and the muscles become weaker, the pain increases even more and each time it is even harder for the person to get back on their feet and function normally forward (Waddell, 2006).
No wonder this method is no longer functional, except in the case of unbearable acute pain and inability to move. Then we are forced to rest for a day or two, but the most important thing in all this is to start moving as soon as possible. Walking is enough to start with, followed by cycling (stationary bike) and swimming (Waddell, 2006).
Figure 1. The site where lumbar back pain may occur.
Our entire movement requires the participation of the spine, and problems with the spine are in most cases the result of multiple wrong loads. The injuries occur over years or even decades, and are influenced by many factors. People are too unaware of how important their spine is. They pay no attention to it, as the pain in it usually only shows up after a few years or decades. Although we are sometimes aware of the problem, we do not do much for our spine. They are not aware of the burdens of irregular movement patterns and the consequences this can have on our lives.
1.2 Core stabilizers and low back pain
Research shows that weak core stabilizers can cause lumbar spine pain. However, people who experience pain can reduce or eliminate the pain with the help of core strengthening exercises. Activating core stabilization muscles is even more effective with later strength and endurance exercises.
1.3 Core stabilizers
Bergmark (1989) divided core muscles into two groups and described them with a clinically applicable concept of local and global muscles. The muscles that run between the pelvis and the chest and attach to the vertebrae at least at one end are counted to the local system. These are mainly deeper lying muscles whose job is to maintain the mechanical rigidity of the spine and control movement between adjacent vertebrae. Global muscles include larger muscles that cross more moving segments and lie more superficially.
Core stabilizers are one of the most important muscles in our body. We are often not even aware of how important they are in our daily activities. Core stabilizers take care of our posture, allow the core to bend and stretch, and take care of the stability of the spine in everyday life (Cao, Schoenfisch, Tan, & Wang, 2013). Strong core stabilizers allow us to distribute the force caused by loads, while protecting our spine from injury. We divide them into local and global muscular system.
The core stabilizers consist of the back muscles, the abdominal muscles (front and side) and the pelvic floor muscles (PFM).
According to Kisner and Colby, stabilizer muscles are defined by role and position.
Core surface muscles
Deep core muscles
– further away from the axis of movement – cross several segments – perform strong contractions
– closer to the axis of movement – attached to each segment of the spine – control the movements of individual segments – composed largely of type 1 muscle fibers (more durable fibers)
The characteristics of the superficial and deep muscles of the core are shown above. It is presented where they are located, what their job is and what these muscles are called.
Figure 2: Abdominal muscles Figure 3: Back muscles
The transverse abdominal muscle (M. transversus abdominis) is the deepest muscle among them and is especially important for maintaining posture. In addition to this muscle, others in this area are shown: the abdominal muscle (M. rectus abdominis), the external oblique abdominal muscle (M. obliquus externus), the inguinal ligament (Inguinal ligament) and the internal oblique abdominal muscle (M. obliquus internus); which has the middle layer removed so that the transverse abdominal muscle can be seen.
Figure 4 shows the pelvic floor muscles. They take care of the correct position of the pelvic organs, and at the same time stabilize the spine.
Core stabilizers have a dynamic control role and are responsible for transmitting large forces from the lower and upper extremities across the core to achieve maximum efficiency and to achieve proper biomechanics of movement ( Sharrock et al., 2011).
Some researchers have described core stabilizers as a double-walled cylinder with the diaphragm at the top, with the abdominal muscles at the front, with the spinal muscles and glutes at the back, and the pelvic floor and hip muscles, which represent the bottom of the cylinder (Richardson, Jill, Hodges, 1999).
The hip and pelvic floor muscles are the foundation of all stabilizers. Hodges (2003) states that core stabilization synergy arises from the pelvic floor muscles and core muscles. The hip muscles, which cover a fairly large area, are involved in stabilizing the core as well as in generating the forces needed to move the lower extremities during sports movement. The imbalance of all the muscles of the above core stabilizers (agonists – antagonists) has a decisive effect on the stability of the core.
1.4. Core stabilizers and sport
Core stability has received considerable attention in recent years in both research and exercise. Thus, most of you, at least recreationally engaged in sports, have probably come across recommendations for strengthening core muscles or often called core stability exercises.
The stability of the corer allows athletes to control body position, create optimal strength and transmit force along the kinetic chain. Core stability is often required for rotational movements or bending, which is required by almost every sport. Research suggests that Core stabilization exercises may be effective in treating back pain due to spinal instability and other clinical diagnoses. Due to the high loads on the lumbar spine during athletic competition and exercise, athletes are likely to be more susceptible to pain due to instability or spinal injury (Joshua Johnson).
What is the difference between core strength and stability? By definition, “power” is the ability to create force at a given motion. The strength of the core thus creates a force during movement, such as getting up or stretching the back, while we speak of the stability of the core when all the muscles of the tcore are statically tense to resist unwanted movements.
2.0 Exercise to strengthen core stabilizers
An exercise program for the strength and stability of the lumbar spine and core can be used as a preventative program or as a rehabilitation program if you are recovering from low back pain or spinal cord injury. (Princeton University, Athletic Medicine, Lumbar / Core Strength and Stability Exercises)
The program includes a section for the stability of local stabilizers, a section for the stability of surface stabilizers and a section for power. Stability training should be done at least five times a week and strength training should be done 3-4 times a week. The program is divided into three levels:
easy,
medium and
difficult.
It is advisable to start with “easy” exercises and complete them before moving to “medium” and these before moving to “Difficult”.
2.1 Instructions and levels of stabilizer training
The quality of the exercise is more important than the amount of exercise performed. This means that the practitioner performs only as many repetitions as he is able to do in the correct technique. The practitioner can move on to a more difficult modification of a particular exercise only when he is able to maintain stability and complete neuromuscular control during the current exercise, which means that the movement is controlled and coordinated. The goal of any workout is to improve intervertebral stability, pelvic stability, and effective movement. The patient has adequate stability of the pelvis and lumbar spine when complex movement patterns such as case squats and lunges, can be performed without excessive movement in the spine. Core stabilization training must be systematic and progressive.
The first phase is called core stabilization by the author (O`Sullivan, 2001) of the article. In the beginning, we need to focus primarily on small movements of the spine and pelvis that improve neuromuscular efficiency and intervertebral stability. The first phase is the cognitive phase, which requires a high level of self-awareness during the performance of exercises with the aim of shrinking only the local part of the stabilizers, without the involvement of global stabilizers. The goal of the first phase is to achieve harmonious contraction and cooperation of the transverus abdominis and multifidus muscles, controlled breathing and a neutral body position.
In the second phase, which the author (O`Sullivan, 2001) cites as core strength, we can already include eccentric and concentric movements of the spine throughout the range of motion. The second phase is the associative phase, where the emphasis is on improving certain movement patterns. Depending on what kind of back pain the practitioner has, certain movement patterns are divided into several component repetitions, which the practitioner performs in a large number of repetitions. It is very important to keep the spine in a neutral position and control the pain. If the practitioner has his spine in a neutral position and there is no pain, the practitioner can also perform movements such as sitting, getting up, lifting and walking. The speed and complexity of the movement should be gradually increased to such an extent that the practitioner can control the complex pattern of movement without pain. The practitioneris also encouraged to do regular aerobic exercise, such as walking, as this will give the muscles a certain tone. This phase of training can last from 8 weeks to four months. At the end of this program, the patients are able to perform complex movements in a controlled manner without any pain.
In the last, third phase, called core force, dynamic stabilization and rotation (Clark, Luccet, Sutton, 2011) can also be included in training. The third phase of training is about automating movements. At this stage, a very low level of attention is required to perform proper motor tasks. The third phase is actually the goal of the entire program. In it, practitioners use dynamic stabilization both in training and in life in everyday tasks.
Figure 5. All three stages of back stabilization training
LMS – local muscles system (O`Sullivan )
In Figure 5, we can see the first, second, and third phases of back stabilization training. The inner circle represents the cognitive phase and its exercises, the middle ring shows the exercises in the associative phase, and in the third or outer ring we can see which tasks in everyday life people use dynamic stabilization. Before each exercise, the practitioner must know exactly what is required of him. We can use the pictorial material to illustrate the exercises. Proper demonstration of the exercise is also highly recommended, where the practitioner can observe the correct execution of the exercise. We have to adapt the explanation of each exercise to each patient. In case of incorrect performance of the exercise, we immediately interrupt it and show the patient the correct version again. If the patient is not able to achieve it, the trainer must find an easier modification of the desired exercise. The conversation between the patient and the trainer is also of great value. Only in this way can the trainer get to know the well-being and feelings of the patient during the implementation of an individual exercise or the entire training program. Here he must pay particular attention to any pain that occurs in the patient.
2.2. Methodology for power development of core stabilizers
In the chapter exercise for developing the strength of core stabilizers, we will describe in three stages exercises that will improve the strength of our stabilizers, and consequently we will be able to reduce or eliminate back pain. We will step up the exercises according to the difficulty, and at the same time add pictorial material.
The first stage or phase involves the activation of local stabilizers. Activation of local stabilizers in the first phase, we focus on the technique of activating the abdominal muscles and developing the strength of the pelvic floor muscles (exercises from 1a to 1d). The absence of pain is very important.
It is followed by the phase of activation of surface stabilizers including static and dynamic exercises. Activation of surface stabilizers in the second phase, we develop the power of the surface muscles, while controlling the local muscles (inner). The exercises are mostly static and are performed in several planes. In the certain exercises, we achieved a small dynamic. The last phase is the stabilization and strengthen of the core during slow and controlled movement.
The eccentric and concentric contractions are performed in all three planes. Movement is slow and controlled. We also used gadgets in the third stage (ball).
2.2.1 Activation of local stabilizers
The first phase is aimed at activating local stabilizers. Since people with low back pain are still unable to withstand the loads required by heavier exercises during this period, this phase is designed to properly activate the muscles of the indoor unit. We will strive for a neutral position of the spine, minimal activity of superficial muscles, and above all, we must ensure the absence of pain.
Figure 6. Three methods to activate the stabilizing musculature in lumbar spine.
Most mentioned techniques for activating abdominal muscles:
(A) drawing-in maneuver in which the patient hollows the abdominal region (“draws” the belly button toward the spine )
(B) abdominal bracing which setting the abdominal muscles results in flaring laterally around the waist
(C) posterior pelvic tilt in which the pelvis is actively tilted posteriorly on the lumbar spine flatness
Retrived from Colby Lynn,Allen Kisner Carolyn: Therapeutic exercises (2012)
Figure 6 shows all three abdominal muscle activation techniques. The drawing-in maneuver also functions to increased intra-abdominal pressure by inwardly displacing the abdominal wall. Because of this the drawing-in is recommended for stabilisation trening (Kisner and Colby ) The patient should first perform it in a lying position (as in the knee 70-90 degrees), and later he should also perform it in a sitting and standing position. The patient should exhale first, then inhale and pull the navel towards the spine, while maintaining tension in the abdominal region. The goal is to increase intra-abdominal pressure, with minimal or even no contraction of the internal oblique.
Figure 7 Checking before a drawing-inmaneuver
Figure 8. Execution of a drawing-in maneuver in a supine position
Figure 9. Execution of a drawing-inmaneuver in the sitting position
Figure 10. Execution of a drawing-in maneuver in the kneeling position
Figure 7 shows the checking if there is a space for the outstretched fingers of one hand between the low back and the base before the execution of the drawing-in maneuver. Figure 8 shows the execution of the drawing-in maneuver in the supine position. Figure 10 also shows the use of the rod. Only this serves to help us achieve a neutral posture of the spine.
The main purpose of drawing-in maneuver (ADIM) is to strengthen a deep muscles, such as the transverse abdominal muscle, the internal oblique muscle, and the external oblique muscle. ADIM is an exercise method that increases abdominal pressure by pulling the abdominal walls inward, allowing the transverse and oblique abdominal muscles to contract. Due to the increased abdominal pressure, training for lumbar core stability is effectively performed.
Patient position
The training may be easiest in lying position in order to use effects of gravity on the abdominal wall. Hook-lying (with 70 to 80 degrees and feet resting on an exercise mat), prone-lying or semireclined position may be used if more comfortable for the patient.
It is important to progress training to sitting and standing position as soon as possible,
Figure 11. Palpation of the transversus abdominis (TA) muscle.
The TA feels like a tense sheet (a bulge is the internal oblique) when performing a gentle drawing-in maneuver.
Retrived from Colby Lynn,Allen Kisner Carolyn, 2012
Procedure
Have the patient assume a neutral spine position and attempt to maintain it while gently drawing in and hollowing the abdominal muscles. Patient have to breath in, breath out, then gently draw the belly button in toward the spine to hollow out the abdominal region . When done properly, there is minimal to no movement of the pelvis (posterior pelvic tilting) , no flaring or depression of the lower rips, no inspiration or lifting of the rib cage, no bulging out of the abdominal wall, and no increased pressure throw the feet.
Abdominal drawing-in maneuver (ADIM) is the main for the strengthening of the deep muscle such as transverses abdominis, internal oblique; and external oblique. ADIM is the exercise method which increases the abdominal pressure by pulling the abdominal walls to the inside that Tra and oblique abdominal are contracted. Because of the increased abdominal pressure, lumbar trunk stability training is effectively accomplished. Also, it induces the muscle contraction that excessive lordosis and tilts of the pelvis are reduced which is effective for the LBP (Kisner and Colby, 2012).
Back pain is one of the more common problems of modern society. The number of people who experience pain in any part of the spine at least once in their lives is increasing. One of the most common is certainly pain in the lumbar region of the back. Today’s lifestyle, where we sit a lot and at the same time have very little time to devote to exercise, is certainly one of the main causes of these pains. Depending on the way of life nowadays, however, these pains will become more and more frequent. Although there are more and more people with low back pain, too few people are still involved in prevention.
Reference
Cao, L., Schoenfisch, W., Tan, S., Wang, J. (2013). Investigation of core muscule function through electromyography activities in healthy young men. Journal of exercise physiology, 16(1), 45-52. Pridobljeno iz http://www.asep.org/asep/asep/JEPonlineFEBRUARY2013_Wang.pdf
Clark, A. M., Lucett, C. S., Sutton, G., B. (Eds.). (2011). NASM Essentials of personal fitness training. United States of America: National Academy of Sports Medicine.
Comerford, M., Jull, G., Richardson, C.G. Toppenberg, R. Techniques for active lumbar stabilisation for spinal protection: a pilot study. Australian Journal of Physiotherapy, 38(2), 105-112.
Kisner C. in Colby L.A., (2007). Therapeutic exercises. Philadelphia: F.A. Davis Company. 38
Kos Golja, M. (2001). Bolečine v križu z revmatološkega vidika. V M. Ivanuša (ur.), Bolečina v križu. (str. 8–11). Novo mesto: Krka.
dr. Robert Košak, dr. med. UKC Ljubljana, Ortopedska klinika ,2010
McGill, S. (2007). Low back disorders. United states: Human kinetics
O`Sullivan P. (2001). Variation in progression of specific back stabilizing exercises. Manual teraphy, 6(1). 3-14. Pridobljeno iz: http://www.back-exercises.com/back-stabilizing-exercises.html
Pori, P., Pistotnik, B., Dolenec, A., Tomažin, K., Štirn, I., Majerič, M. (2013). Športna rekreacija. Ljubljana: Športna unija Slovenije, Fundacija za šport.
Richardson, C.A., Jull, G.A. in Richardson, B.A. (1995). A dysfunction of the deep abdominal muscles exists in low back pain patients. V: Proceedings of World Confederation of Physical Therapists, Washington.
Sharrock C, Cropper J, Mostad J, Johnson M and Malone T. A pilot study of core stability and athletic performance: Is there a relationship? The International Journal of Sport s Physical Therapy,
Waddell, G. (1999). The back pain revolution. Edinburgh: Churchill Livingstone.
1. Vaje za krepitev mišic medeničnega dna (PFM) v ležanju na hrbtu in boku, težavnost : lahko.
Vaja
Opis
Začetni položaj
Potek vadbe
1a
Ležanje na hrbtu, ena noga upognjena, druga pa iztegnjena, stabilen ledveni del hrbta, izvedemo drawing-in manever. Dvigujemo iztegnjeno nogo ( brez bolečine).
Ležimo na hrbtu, ena noga je upognjena, druga pa iztegnjena,stabilen ledveni del hrbta, izvedemo drawing-in manever. Z iztegnjeno nogo, krožimo (brez bolečine)
Ležimo na boku, ena noga je upognjena, druga pa iztegnjena , stabilen ledveni del hrbta, izvedemo drawing-in manever. Iztegnjeno nogo dvigujemo (brez bolečine)
Ležimo na boku, ena noga je upognjena, druga pa iztegnjena, stabilen ledveni del hrbta, izvedemo drawing-in manever. Z iztegnjeno nogo krožimo (brez bolečine)
Ponovitev : število Pponovitev vaje, če obe je L+D , je število ponovitev z vsako nogo oz, roko.
Trajanje : trajanjevaje v sekundah oziroma zadrževanje pozicije.
Odmor :odmor med vajo v sekudah.
Dni v tednu : število vadbenih dni v tednu.
Obe(L/D) : Leva ali Desna ali obe nogi/roki.
Trajanje obdobja aktiviranja lokalnih stabilizatorjev ni časovno določeno. To je odvisno od pacienta, saj je aktivni čas prve faze pri pacientih različen. Ljudje se razlikujemo po svojih sposobnostih. Nekateri bodo tehnike za aktivacijo obvladali prej, drugi kasneje. Vendar je za aktiviranje trebušnih mišic in mišic medeničnega dna priporočljivo izvajati vadbo vsaj 5 krat na teden in štiri tedne. Le pravilna izvedba drawing-in manevra nam lahko omogoči varno izvajanje vaj za stabilizacijo trupa v naslednjih fazah, kar bo vodilo do zmanjšanja bolečin v križu. Zelo pomemben je tudi razvoj mišic medeničnega dna, čemur večina ljudi in terapevtov posveča premalo pozornosti.
2. Vaje za PFM leže na hrbtu z uporabo žoge, težavnost : srednje.
Vaja
Opis
Začetni položaj
Potek vadbe
1e
Ležite na hrbtu, upognite noge (70-90 st.) , stabilna ledvena regija, izvedite drawing-in manever, stisnite žogo s koleni in pritisnite roke na podlago. Oprema: žoga.
Ponovitve 1 : 5 x Trajanje 2 : 5 sek Odmor 3 : 5 sek Dni v tednu 4: 4
1f
Ležite na hrbtu, upognite noge (70-90 st.), stabilna ledvena regija, izvedite Drawing-in manever , stisnite žogo s koleni in z rokami potiskajte noge od sebe. Oprema: žoga.
Ponovitve 1 : 5 x Trajanje 2 : 5 sek Odmor 3 : 5 sek Dni v tednu 4: 4
1g
Ležite na hrbtu, upognite noge, stabilna ledvena regija, izvedite drawing-in manever, stisnite žogo s koleni in dvignite roke na kolena. Oprema: žoga.
Ponovitve 1 : 5 x Trajanje 2 : 5 sek Odmor 3 : 5 sek Dni v tednu 4: 4
3.. Vaje za stabilizacijo trupa v klečečem in bočnem položajutežavnost : srednje.
Vaja
Opis
Začetni položaj
Potek vadbe
2a
Opora je na dlaneh in kolenu ene noge, druga noga je iztegnjena, stabilen ledveni del hrbta, izvedemo drawing-in manever. Dvigujemo iztegnjeno nogo. Pripomoček : palica za nevtralno lego hrbtenice in pas za pritrditev
Opora je na dlaneh in kolenu ene noge, druga noga je iztegnjena, stabilen ledveni del hrbta, izvedemo drawing-in manever. Dvigujemo iztegnjeno nogo in nasprotno roko. Pripomoček : palica za nevtralno lego hrbtenice in pas za pritrditev
Glavni namen tega prispevka je oblikovanje programa vadbe za razvoj moči in stabilnosti trupa za vse, ki imajo bolečine v križu ali želijo izboljšati moč stabilizatorjev trupa. Po pregledu literature novejših raziskav na to temo sem razvil program vadbe, ki pomaga zmanjšati in v nekaterih primerih odpraviti bolečino v križu, ojačati stabilizatorje trupa in omogočiti kvalitetno življenje brez bolečin.
Dodana je razlaga mišic, pomembnih za ledveni del hrbta in trup telesa. Opisane so mišice medeničnega dna, ki skrbijo za pravilen položaj medeničnih organov in hkrati stabilizirajo hrbtenico. Program je sistemsko razdeljen na tri zaporedne segmente. Za vsak segment je pripravljen osnovni in naprednejši sklop vaj, da se upošteva razlike v stopnji telesne pripravljenosti vadečega.
1.0 Bolečina v križu
Bolečina v ledvenem predelu hrbtenice je najbolj pogosta bolečina gibal pri človeku. Devetdeset odstotkov odraslih oseb v času svojega življenja vsaj enkrat ali tudi večkrat začuti značilno bolečino v križu. Petdeset odstotkov ljudi ima v aktivnem (delovnem) življenjskem obdobju bolečino v križu vsaj enkrat na leto. Bolečina v ledvenem predelu hrbtenice je lahko akutna, subakutna ali kronična. (Robert Košak, 2010, UKC)
Nekatere raziskave ( McGill, 2007) potrjujejo, da so ljudje z bolečinami v križu v preteklosti imeli povečan obseg pasu, zmanjšano mišično zmogljivost (zlasti mišic trupa) in zmanjšano kontrolo gibanja. McGill v svoji knjigi (2007) navaja vzroke poškodb in predlaga za zmanjšanje specifičnih poškodb z naslednja priporočila:
odprava stresorjev ki so vzrok poškodbe ledvenega dela hrbtenice,
izvajanje aktivnosti za zdravo podporno tkivo,
idealna drža pri sedenju je tista, ki se nenehno spreminja in in ob tem preprečuje preobrementev tkiva,
pri ljudeh nagnjenih k bolečinam v križu obstajata dve vrsti dejavnikov tveganja:
dejavniki, ki so vezani na osebo (npr. slaba mišična vzdržljivost ) in
dejavniki, ki so vezani na zahteve nalog, ki jih oseba opravlja (npr. dvigovanje uteži, prelaganje tovora itd.).
Pri bolečini v križu je treba ločiti med :
akutno bolečino – bolečina, ki traja 6 tednov ali manj;
subakutno bolečino – bolečina, ki traja od 6 do 12 tednov;
kronično bolečino – bolečina, ki traja več kot 12 tednov.
Prepričanje, da je za zdravljenje in odpravo bolečin v križu nujen počitek ali ležanje dokler bolečine ne minejo, se je pokazalo za škodljivega. Saj ležanje v postelji več kot dva dni samo poslabša stanje, ker oslabi kosti in mišice, kar zmanjša fizično moč telesa, ki postane neelastično. Oseba lahko zapade v depresijo in bolečina se še poveča in vse težje je okrevanje (Waddell, 2006). Zato ta metoda ni koristna, razen v primeru nevzdržne akutne bolečine in nezmožnosti gibanja. Potem smo prisiljeni počivati nekaj dni, a najpomembnejše pri vsem tem je, da čim prej začnemo s terapevtskimi vajami in gibanjem (Waddell, 2006).
Slika 1. Mesto, kjer se lahko pojavijo bolečine v ledvenem delu hrbta.
Celotno naše gibanje se prenaša na hrbtenico, kjer se v primeru večkratnih preobremenitev pojavijo poškodbe po več letih ali celo desetletjih. Ker se premalo zavedamo, kako pomembna je naša hrbtenica, na to nismo pozorni. Bolečina v hrbtenici se ponavadi pokaže šele čez nekaj let. Čeprav se včasih težav zavedamo, za svojo hrbtenico ne naredimo dovolj.
1.2 Stabilizatorji trupain bolečina v križu
Iz raziskav sledi, da so lahko šibki stabilizatorji trupa vzrok bolečin v ledvenem delu hrbtenice. Ljudje, ki se srečujejo z bolečinami pa lahko bolečino zmanjšajo ali odpravijo s pomočjo vaj za ojačanje stabilizatorjev trupa. Aktivacija mišic za stabilizacijo trupa je še učinkovitejša s kasnejšimi vajami za moč in vzdržljivost.
1.3Stabilizatorji trupa
Bergmark (1989) je mišice trupa razdelil v dve skupini in jih opisal s klinično uporabnim konceptom lokalnih in globalnih mišic. Mišice, ki potekajo med medenico in prsnim košem in se vsaj na enem koncu priraščajo na vretenca, prištevamo k lokalnemu sistemu. To so predvsem globlje ležeče mišice, katerih naloga je vzdrževanje mehanske togosti hrbtenice in nadzor gibanja med sosednjimi vretenci. H globalnim mišicam prištevamo večje mišice, ki prečijo več gibljivih segmentov in ležijo bolj površinsko. Aktivacijski vzorci globalnih mišic kažejo na njihovo kombinirano vlogo stabilizatorjev trupa, generatorjev navorov in prenašalcev obremenitve med spodnjimi udi, medenico, hrbtenico, trupom in zgornjimi udi. Obe skupini ves čas delujeta vzajemno, pri čemer globalni sistem uravnoteži velike zunanje sile do te mere, da jih lahko lokalni sistem obvlada.
Stabilizatorji trupa so ena najpomembnejših skupin mišic v našem telesu. Pogosto se niti ne zavedamo, kako pomembni so pri naših vsakodnevnih aktivnostih. Stabilizatorji trupa skrbijo za našo držo, omogočajo upogibanje in raztezanje trupa ter skrbijo za stabilnost hrbtenice v vsakdanjem življenju (Cao, Schoenfisch, Tan in Wang, 2013). Močni stabilizatorji trupa nam omogočajo, da silo, ki jo povzročajo obremenitve, porazdelimo, hkrati pa hrbtenico zaščitimo pred poškodbami. Delimo jih na lokalni in globalni mišični sistem. Stabilizatorji trupa so sestavljeni iz hrbtnih mišic, trebušnih mišic (spredaj in ob strani) in mišic medeničnega dna (MMD).
Po Kisner in Colby so mišice stabilizatorjev opredeljene glede na vlogo in lego.
Površinske mišice trupa
Globoke mišice trupa
– bolj oddaljene od osi gibanja – prečkajo več segmentov – izvajajo gibanje – močne kontrakcije
– bližje osi gibanja – pripete na vsak segment hrbtenice – kontrolirajo gibe posameznih segmentov – v veliki meri sestavljene iz mišičnih vlaken tipa 1 (bolj vzdržljiva vlakna)
V tabeli so prikazane značilnosti površinskih in globokih mišic trupa. Predstavljeno je, kje se nahajajo, kaj je njihova naloga in kako se te mišice imenujejo.
Slika 2: Trebušne (abdominalne) mišice Slika 3: Hrbtne mišice
Prečna trebušna mišica (Muscle transversus abdominis) je najgloblja mišica med njimi in je posebej pomembna za ohranjanje drže. Poleg te mišice so prikazane še ostale v tem predelu: prema trebušna mišica (M. rectus abdominis), zunanja poševna trebušna mišica (M. obliquus externus), dimeljski ligament (Inguinal ligament) in notranja poševna trebušna mišica (M. obliquus internus) , ki ima odstranjeno srednjo plast, da je lahko vidna prečna trebušna mišica.
Stabilizatorji trupa so odgovorni za prenos sil na trup iz zgornjih in spodnjih okončin za doseganje največje učinkovitosti gibanja ( Sharrock et al., 2011).
Nekateri raziskovalci so stabilizatorje trupa opisali kot dvostenski valj z diafragmo na vrhu, s trebušnimi mišicami spredaj, s hrbteničnimi in zadnjičnimi mišicami ter mišicami medeničnega dna, ki predstavljajo dno valja (Richardson, Jull, Hodges, 1999). Sinergija stabilizacije trupa izvira iz mišic medeničnega dna in mišic trupa ( Hodges , 2003).
1.3Stabilizatorji trupa in šport
Stabilnost trupa je v zadnjih letih deležna precejšnje pozornosti tako na raziskovalnem področju, kakor tudi na področju vadbe. Tako se večina, ki se vsaj rekreativno ukvarja s športom, verjetno srečala s priporočili za krepitev mišic trupa ali pogosto imenovanimi vajami za stabilnost jedra.
Stabilnosti trupa omogoča športnikom nadzor nad položajem telesa, ustvarjanje optimalne moči in prenos sile po kinetični verigi. Stabilnost trupa je pogosto potrebna pri rotacijskih gibih ali pri upogibanju, kar zahteva skoraj vsak šport. Raziskave kažejo, da so lahko vaje za stabilizacijo trupa učinkovite pri zdravljenju bolečin v hrbtu zaradi nestabilnost hrbtenice in drugih kliničnih diagnoz. Zaradi velikih obremenitev ledvenega dela hrbtenice med atletskim tekmovanjem in vadbo so atleti verjetno bolj dovzetni za bolečino zaradi nestabilnosti ali poškodbe hrbtenice (Joshua Johnson ).
Kakšna je razlika med močjo in stabilnostjo trupa? Po definiciji je “moč” sposobnost ustvarjanja sile ob danem gibanju. Moč trupa torej ustvarja silo med gibanjem, kot je vstajanje ali raztezanje hrbta, medtem ko o stabilnosti trupa govorimo takrat, ko se vse mišice trupa statično napete, da se upremo neželenim gibom.
2.0 Vadba za krepitev stabilizatorjev trupa
Iz raziskav stabilizatorjev trupa sledi, da so lahko šibki stabilizatorji trupa vzrok bolečin v ledvenem delu hrbtenice. Ljudje, ki se srečujejo z bolečinami, pa lahko bolečino zmanjšajo ali odpravijo s pomočjo vaj za ojačanje stabilizatorjev trupa.
2.1 Navodila in nivoji treninga za stabilizacijo trupa
Kakovost vaje je pomembnejša od števila izvedenih vaj. To pomeni, da pacient izvede le toliko ponovitev, kolikor je zmožen ob pravilni izvedbi vaje. Pacient lahko preide na zahtevnejšo vaje šele, ko je sposoben med trenutno vajo ohraniti stabilnost in popolno kontrolo izvedbe, kar pomeni, da je gibanje nadzorovano in usklajeno. Cilj vsakega treninga je izboljšati stabilnost hrbtenice in medenice za učinkovito gibanje. Pacient ima ustrezno stabilnost medenice in ledvene hrbtenice, kadar je mogoče izvajati zapletene vzorce gibanja, kot so počepi, brez pretiranega gibanja v hrbtenici. Vadba za stabilizacijo trupa mora biti sistematična in postopna.
Prvo fazo imenujemo stabilizacija trupa (O`Sullivan, 2000). Ta faza je tudi kognitivna faza, ki zahteva visoko stopnjo samozavedanja med izvajanjem vaj z namenom krčenja samo lokalnih stabilizatorjev, brez sodelovanja globalnih stabilizatorjev. Cilj prve faze je doseči harmonično krčenje in sodelovanje mišic transversus abdominis in multifidus, nadzorovano dihanje in nevtralen položaj telesa.
Druga faza vključuje vaje za moč trupa (O`Sullivan, 2000). Tu že lahko vključimo ekscentrične in koncentrične gibe hrbtenice v celotnem obsegu gibanja. Druga faza (8) je tudi asociativna faza, kjer je poudarek na izboljšanju določenih gibalnih vzorcev. Glede na to, kakšne bolečine v hrbtu ima pacient, so določeni gibalni vzorci razdeljeni na več sestavljenih ponovitev, ki jih izvaja v velikem številu ponovitev. Zelo pomembno je, da hrbtenico držite v nevtralnem položaju in nadzorujete bolečino. Če ima pacient hrbtenico v nevtralnem položaju brez bolečin, lahko izvaja vaje, kot so sedanje, vstajanje, dvigovanje lažjega bremena (lat gym machine) in hoja. Hitrost in zahtevnost gibanja se postopoma povečuje do te mere, da lahko pacient izvaja gibanje brez bolečin. Pacient poleg vaj izvaja redno aerobno vadbo: hoja, hoja s palicami, vožnja s kolesom (predvsem sobno) in tako pridobi večji mišični tonus.
V zadnji, tretji fazi, imenovani sile trupa, je v trening mogoče vključiti tudi dinamično stabilizacijo in rotacijo (Clark, Luccet, Sutton, 2011). Tretja faza treninga je namenjena tudi avtomatizaciji gibov. V tej fazi je izvajanje pravilnih gibalnih nalog že samodejno z osredotočenostjo na količino vadbe. Tretja faza je pravzaprav cilj celotnega programa. V njem izvajalci uporabljajo dinamično stabilizacijo tako pri treningu kot v življenju pri vsakdanjih nalogah.
Slika 5. Vse tri faze treninga stabilizacije
LMS – lokalni mišični sistem hrbtnih mišic ( O`Sullivan )
Na sliki 5 lahko vidimo prvo, drugo in tretjo fazo treninga stabilizacije hrbta. Notranji krog predstavlja kognitivno fazo in njene vaje, srednji obroč prikazuje vaje v asociativni fazi, v tretjem ali zunanjem obroču pa lahko vidimo opravila v vsakdanjem življenju, kjer ljudje uporabljajo dinamično stabilizacijo. Pred vsako vajo mora izvajalec natančno spoznati vaje. Slikovno in video gradivo je dodano za predstavitev vaj. Priporočljiv je tudi ustrezen prikaz vaje, kjer lahko pacient opazuje pravilno izvedbo vaje. Lahko je on-line ali neposredno s pomočjo terapevta. V tem primeru moramo razlago vsake vaje prilagoditi vsakemu pacientu. Pravilen prikaz vaje je nujen za pacientovo pravilno izvedbo.
2.2. Metodologija za razvoj moči stabilizatorjev trupa
V poglavju vaje za razvoj moči stabilizatorjev trupa so v treh stopnjah opisane vaje za izboljšanje moči stabilizatorjev trupa in s tem zmanjšali ali odpravili bolečine v hrbtu. Vaje so stopnjevane glede na težavnost in dodano je slikovno in video gradivo.
Prva stopnja ali faza vključuje aktiviranje lokalnih stabilizatorjev. V prvi fazi se osredotočimo na tehniko aktiviranja mišic medeničnega dna in razvoja moči mišic medeničnega dna in trebušnih mišic (vaje od 1a do 1d). Zelo pomembna pa je odsotnost bolečine .
Sledi faza aktiviranja površinskih stabilizatorjev s statičnimi in dinamičnimi vajami. V fazi aktiviranja površinskih stabilizatorjev razvijamo moč površinskih mišic, hkrati pa nadzorujemo notranje mišice. Vaje so večinoma statične z majhno dinamiko. (vaje od 2a do 2c ).
V tretji fazi se izvajajo ekscentrične in koncentrične kontrakcije v vseh treh ravninah. Gibanje je počasno in nadzorovano. V tretji fazi smo uporabili tudi pripomočke (žogo). (vaje od 3a do 3e)
2.2.1 Aktiviranje lokalnih stabilizatorjev
Prva faza je namenjena aktiviranju lokalnih stabilizatorjev. Ker ljudje z bolečinami v ledvenem delu hrbta v tem obdobju še vedno ne morejo prenesti obremenitev, ki jih zahtevajo težje vaje, je ta faza zasnovana tako, da pravilno aktivira mišice notranje enote. Prizadevali si bomo za nevtralen položaj hrbtenice, minimalno aktivnost površinskih mišic, predvsem pa moramo zagotoviti odsotnost bolečine
.
Slika 6. Prikaz tehnik aktivacije trebušnih mišic in mišic medeničnega dna
Pridobljeno iz Colby Lynn,Allen Kisner Carolyn: Therapeutic exercises (2012).
Največkrat omenjene tehnike za aktiviranje trebušnih mišic in mišic medeničnega dna:
(A) drawing-in manever, pri katerem pacient upogne trebušni del (“potegne” popek proti hrbtenici),
(B) abdominalno napenjanje ali stisk vseh abdominalnih mišic in
(C) nagib medenice navzdol, tako da se izravna ledvni del hrbtenice.
Slika 6 prikazuje vse tri tehnike aktivacije trebušne mišice in mišic medeničnega dna. Drawing-in manever deluje tudi na povečan intraabdominalni tlak, tako da premakne trebušno steno navznoter. Zaradi tega je drawing-in manever priporočljiv za stabilizacijski trening (Kisner in Colby, 2012). Pacient mora drawing-in manever najprej izvesti v ležečem položaju (kot v kolenu 70-90 stopinj), kasneje pa ga izvaja tudi v sedečem in stoječem položaju.
Cilj drawing-in manevera je zvišanje intraabdominalnega tlaka z minimalnim krčenjem ali brez krčenja notranje poševne muskulature.
Pri treningu mišic medeničnega dna je zelo pomembno, da vaje izvajate pravilno. Pacient mora imeti občutek, kot da želi stisniti zadnjično odprtino in ustaviti uhajanje vetrov in hkrati zadrževati curek urina. Pri treningu mišic medeničnega dna spreminjamo tako začetni položaj vadečega kot količino izvedenih vaj. Na začetku vadeči leži na hrbtu s poskrčenimi nogami (koleno upognjeno med 70-90 stopinj) (slika 6), kasneje pa se lahko premakne na oporo, kjer sedi (slika 7) in stoji z dlanmi na zadnjici (Pori et.al, 2013).
Slika 7. Preverjanje pred a drawing-in manevrom
Slika 8. Izvedba a drawing-in manevra ležečem položaju
Slika 9. Izvedba drawing-in manevra v sedečem položaju
Slika 10. Izvedba drawing-in manevra v klečečem položaju
Na sliki 7 je prikazano preverjanje, ali je prostor za iztegnjene prste ene roke med spodnjim delom hrbta in podlago pred izvedbo drawing-in manevra. Če ni prostora je potrebno podložiti tanko zvito brisačo. Slika 8 prikazuje izvedbo drawing-in manevra v ležečem položaju. Na sliki 10 je prikazana tudi uporaba palice, ki nam služi kot pomoč pri doseganju pravilne drže hrbtenice. Le ta nam pomaga, da dosežemo nevtralno držo hrbtenice.
Glavni namen drawing-in manevra (ADIM) je krepitev globokih mišic, na primer prečne trebušne mišice, notranje poševne in zunanje poševne mišice. ADIM je vadbena metoda, ki poveča trebušni pritisk tako, da trebušno stene povleče v notranjost in tako omogoči krčije prečne in poševne trebušne mišice. Zaradi povečanega trebušnega tlaka se učinkovito izvaja trening za stabilnost ledvenega dela trupa.
Položaj pacienta
Vadba je najlažja v ležečem položaju, pri katerem se izkoristi učinek gravitacije na trebušno steno. Kot v kolenih naj bo med 70 in 80 stopinjami z nogami, naslonjenimi na podlogo za vadbo. Polležeč položaj se lahko uporabi, če je bolniku bolj udobno. Pomembno je, da trening čim prej napreduje v sedeč in stoječ položaj.
Postopek
Pacient naj zavzame nevtralni položaj hrbtenice in ga poskuša ohraniti, medtem ko nežno vleče in upogiba trebušne mišice. Pacient naj vdihne, izdihne, nato nežno potegne popek proti hrbtenici, da upogne trebušni del, hkrati pa ohranja napetost v predelu trebuha. Če je postopek pravilno opravljen pomeni, da ni gibanja medenice ali je minimalno ( zadnji nagib medenice), nobenega upogibanja reber, nobenega dvigovanja ali napenjanja reber in nobenega povečanega pritiska na stopala. (Kisner in Colby, 2012).
Slika 11. Palpacija mišice transversus abdominis (TA), TA se pri nežnem drawing-in manevru čuti kot napeta plahta (izbočena je notranja poševna mišica).
Bolečine v hrbtenici so ena najpogostejših težav sodobnega človeka. Število ljudi, ki se vsaj enkrat v življenju reča z bolečino v katerem koli delu hrbtenice, narašča. Ena najpogostejših je zagotovo bolečina v ledvenem delu hrbta. Današnji življenjski slog, kjer veliko sedimo in se malo gibljemo, hkrati pa imamo zelo malo časa za vadbo, je den glavnih vzrokov za te bolečine. Glede na današnji način življenja pa bodo te težave vse pogostejše. Ta program je pomemben tudi za preventivo, da bi bi vključil čim več ljudi še predno se pojavi bolečina v križu.
Viri
1. Cao, L., Schoenfisch, W., Tan, S., Wang, J. (2013). Investigation of core muscule function through electromyography activities in healthy young men. Journal of exercise physiology, 16(1), 45-52. Pridobljeno iz http://www.asep.org/asep/asep/JEPonlineFEBRUARY2013_Wang.pdf
3. Comerford, M., Jull, G., Richardson, C.G. Toppenberg, R. Techniques for active lumbar stabilisation for spinal protection: a pilot study. Australian Journal of Physiotherapy, 38(2), 105-112.
8. O`Sullivan P. (2000). Lumbar segmental `instability’: clinical presentation and specific stabilizing exercise management, http://fitnessmais.com.br/download/avaliacao-fisica/estabilizacao-01.pdf
9. Pori, P., Pistotnik, B., Dolenec, A., Tomažin, K., Štirn, I., Majerič, M. (2013). Športna rekreacija. Ljubljana: Športna unija Slovenije, Fundacija za šport.
10. Richardson, C.A., Jull, G.A. in Richardson, B.A. (1995). A dysfunction of the deep abdominal muscles exists in low back pain patients. V: Proceedings of World Confederation of Physical Therapists, Washington.
11. Sharrock C, Cropper J, Mostad J, Johnson M and Malone T. A pilot study of core stability and athletic performance: Is there a relationship? The International Journal of Sport s Physical Therapy,
12. Waddell, G. (1999). The back pain revolution. Edinburgh: Churchill Livingstone.











 1- stisnite zadnjico, oblikujte pravi položaj deske v ravni črti od prstov, skozi boke, do vratu
1- stisnite zadnjico, oblikujte pravi položaj deske v ravni črti od prstov, skozi boke, do vratu